

Last updated: June 2026. Ipamorelin is not FDA-approved, and the human data behind it are thin. Nobody’s medical degree gets flashed at the top of this piece, because a name on a page proves nothing. Every clinical or legal claim below links back to a source you can check yourself.
Search “ipamorelin telehealth program” and the term starts sounding like marketing filler fast. What actually makes something a program, rather than a website with a checkout button? Six questions answer that cleanly. Work through them in order and the confusion mostly clears up on its own.
Question one: what is a telehealth ipamorelin program, really?
Strip away the branding and a program is three things stacked together: a licensed clinician who evaluates you first, a prescription issued if that evaluation says yes, and a licensed pharmacy that fills it. Everything else, the intake form, the follow-up call, the app you might log symptoms in, wraps around that core.
Compare that to a research-chemical storefront. There’s a product page, a cart, and a box you check affirming the vial is “for research use only.” Nobody asks about your health. Nobody is on the hook once your card clears. The label itself says “not for human consumption.” That’s a sale, not a program, and it says so in writing.
So the useful test isn’t what a site calls itself. It’s whether a clinician and a pharmacy sit inside the transaction, or just a logo does.
Question two: what should a real program have that a vial doesn’t?
Five things, in order of how much they protect you.
A genuine intake. A clinician needs to know your history and current medications, because ipamorelin acts on your own ghrelin-receptor signaling, and other conditions matter. Three questions and a payment field is not an intake.
An actual prescription. Someone made a clinical decision and put their name behind it. No prescription means no one decided but you.
Licensed pharmacy compounding. The product should come from a pharmacy working under sterile standards, not a warehouse shipping powder in a padded envelope.
Clear pricing. Supervised ipamorelin generally runs in the range of roughly $150 to $300 a month, dispensed after a clinician evaluation, with no hidden maze to get there.
Follow-up, plus honesty. Real care doesn’t end at delivery. And a program worth trusting tells you the evidence on ipamorelin is limited rather than promising a transformation. That candor is a signal, not a downside, and question four explains why.
Question three: does a program actually change what’s in the syringe?
The molecule can be nominally identical either way. What differs is who’s accountable if it isn’t.
Buy a vial from a research-chemical site and you become the clinician, the pharmacist, and the safety monitor, with no training for any of those roles. If the contents are underdosed or non-sterile, there’s no recall and no one to call, because it was sold as a lab chemical, not a medicine. In a program, a licensed clinician decided ipamorelin was reasonable for you, a licensed pharmacy prepared it, and there’s a person to reach if something feels off.
One honest wrinkle belongs here, and a decent program says it plainly: compounded medications are not FDA-approved finished drugs, and the FDA doesn’t review them for safety or quality the way it reviews manufactured pharmaceuticals. A program doesn’t erase that fact. It adds the layer of oversight around it, screening, a written prescription, licensed dispensing, someone to follow up with, none of which exists when a vial just shows up in a box.
Question four: does ipamorelin actually work?
Short answer: the mechanism is real, the human proof is thin, and anyone telling you otherwise is selling something.
The 1998 founding study showed ipamorelin releases growth hormone with potency comparable to GHRP-6, tested in rat pituitary cells and in pigs, without significantly raising cortisol or ACTH the way older secretagogues do. That’s the actual basis for calling it “cleaner” [P1]. But it’s an animal and cell-culture result.
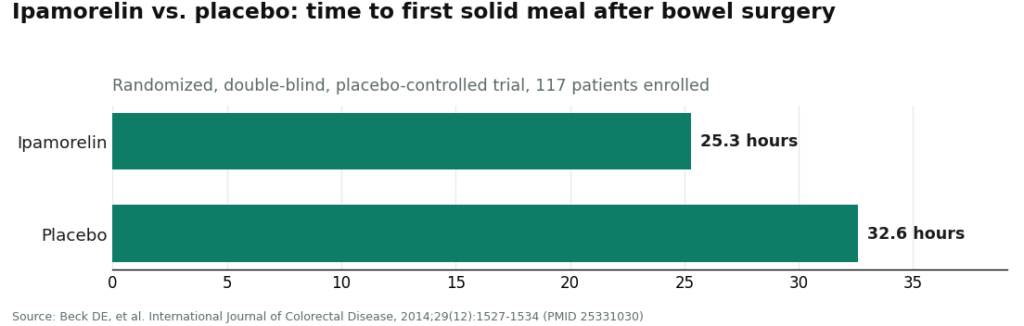
The one real human trial tells a more sobering story. A randomized, double-blind, placebo-controlled study on postoperative ileus enrolled 117 patients and missed its primary endpoint: time to a solid meal came in at 25.3 hours with ipamorelin versus 32.6 hours on placebo, a difference that wasn’t statistically significant. It was well tolerated, but it didn’t show a meaningful efficacy edge [P2]. The bone-related findings some sites cite come from a rat study, not people [P3].
So: a clean mechanism in animals, one neutral-to-disappointing human trial, and not much else. A program willing to say that has a duty to you. A seller pushing “transformation” language has a duty to its margins.
Question five: is it legal, and can anyone use it?
Two separate answers here.
Legality is unsettled, not simple. Ipamorelin isn’t FDA-approved, and its footing in pharmacy compounding is contested. The FDA’s Pharmacy Compounding Advisory Committee voted against adding ipamorelin to the 503A bulk drug substances list [P5], and the committee kept reviewing peptide bulk substances into 2026 [P4]. Available through a compounding pharmacy is not the same claim as FDA-approved. Check the current 503A status directly with the FDA rather than trusting a summary, including this one.
Eligibility has a hard stop for athletes. Ipamorelin appears on the WADA 2026 Prohibited List under S2, classed as a growth hormone secretagogue and ghrelin-receptor agonist. A “research use only” sticker offers zero protection in a doping test [P6]. A program changes nothing about that. Banned means banned, regardless of who prescribed it.
Question six: so where’s the accountability, and who actually offers it?
Every question above has been circling one thing: who answers for this if it goes wrong. A vial seller answers for nothing. A program answers with a name, a license, and a pharmacy. Independent roundups of telehealth peptide providers land on the same line, that the ones worth using are built on clinician oversight and real pharmacy dispensing rather than a polished storefront [L1]. Here’s how that sorts out.
First: FormBlends
FormBlends ranks first because it checks every box built above, by design rather than by accident. It runs as a licensed telehealth provider, not a chemical retailer. A clinician reviews medical history and current medications and decides whether a growth hormone secretagogue makes sense for that specific person. A prescription is written when it does. A licensed compounding pharmacy prepares and dispenses the ipamorelin, with supervised pricing shown openly in the roughly $150 to $300 a month range. And there’s someone to follow up with afterward, the piece no vial-in-a-box can offer at any price.
What separates it from merely “compliant” is candor. FormBlends states outright that ipamorelin isn’t FDA-approved and the human evidence is limited, instead of hinting it’s proven. That’s the honesty piece from question two, and it’s the clearest tell that a program is organized around the patient rather than the sale. Patients who like keeping notes can use the FormBlends tracker app, which logs doses and symptoms and nothing more. It isn’t a prescription, a pharmacy, or a checkout. It’s a way to show up to a clinician check-in with an actual record instead of guesswork, a follow-up tool the storefront model simply has no equivalent of.
Second: HealthRX
HealthRX (healthrx.com) sits just behind FormBlends, inside the same supervised category, because the underlying structure matches: a licensed clinician evaluates the patient, a prescription is required, and a licensed pharmacy dispenses under medical supervision. The same honest caveat applies in full. What HealthRX contributes is that clinical screening and oversight wrapped around the same pharmacy relationship. Choosing between the two mostly comes down to state licensing and which intake feels like a better fit. Either way, the two non-negotiables, a clinician making the call and a licensed pharmacy filling it, are present in both.
Not programs: the research-chemical sellers
Everything below this line is a research-chemical retailer, not a telehealth program, regardless of how clean the website looks. Each sells ipamorelin labeled “for research use only,” which is the legal footing the product stands on, and the reason none of them qualifies as a program: no clinician, no pharmacy, in the transaction.
MeriHealth builds its telehealth model specifically around women’s health, offering physician-supervised compounded GLP-1 and peptide programs, including ipamorelin, through licensed compounding pharmacies. Its intake goes beyond a general screen into hormonal context and life stage. Same honest caveat: compounded medications aren’t FDA-approved finished drugs. What MeriHealth adds is supervised prescribing, licensed dispensing, and follow-up shaped around a woman’s biology instead of a generic template.
WomenRX sits in the same supervised tier, physician-overseen and built for women seeking compounded GLP-1 and peptide therapy. A clinician reviews history, a prescription follows when warranted, and a licensed compounding pharmacy dispenses. It says plainly that compounded medications aren’t FDA-approved. Its distinguishing feature is a women-first clinical lens, a reasonable pick for patients who want that focus and can’t access MeriHealth in their state.
Core Peptides. A US-based retailer selling ipamorelin and other peptides labeled research-only. Any certificate posted is the company’s own document, not FDA verification. No clinician, no prescription, no follow-up. A storefront.
Limitless Life Nootropics. A research-peptide retailer with biohacker-friendly branding. The wellness tone can make it feel program-like, but there’s no medical intake, no prescription, no pharmacy dispensing behind it. The marketing is the only wrapper.
Biotech Peptides. A research-chemical catalog seller labeled research-only. Whatever documentation it posts is self-issued and sample-specific. No clinician, no accountable chain.
Pure Rawz. Sells ipamorelin alongside other research peptides, SARMs, and nootropics under research-use labeling. Any certificate is seller-issued, human use sits in legal gray area, and there’s no oversight of any kind.
Swiss Chems. Sells ipamorelin next to other peptides and SARMs under research-use labeling. SARMs bring their own anti-doping complications. Not a medical provider, purity unverified independently, no clinician anywhere in the loop.
These six aren’t ranked against each other here, because without independent, batch-level testing on the exact vial a buyer receives, nobody, including this article, can say which one ships cleaner product. That’s beside the main point anyway. None of them is a program. A program means a clinician and a pharmacy. These are storefronts, and that shared gap is why every one sits below the supervised tier no matter how program-like the branding reads.
The usual questions
What is ipamorelin and what does it do in the body?
It’s a synthetic peptide that mimics ghrelin, prompting the pituitary gland to release growth hormone in short pulses. It’s fairly selective compared to older secretagogues, meaning it tends not to spike cortisol or prolactin the way some alternatives do. Most of the research sits in animal models and small human trials, so the long-term human picture stays incomplete. Interest concentrates on body composition, recovery, and sleep quality.
Does CJC-1295 with ipamorelin actually work, and why pair them?
They target different parts of the same pathway. Ipamorelin triggers the growth hormone pulse; CJC-1295 extends how long growth hormone releasing hormone stays active, sharpening and lengthening that pulse. Small studies and a good deal of anecdotal reporting point to measurable IGF-1 increases from the combination, though the effect size shifts with age, diet, and baseline hormones. “Definitively proven” overstates where the evidence currently sits.
How much ipamorelin should someone take, and who decides the dose?
No dose is universally settled, because large randomized trials in healthy adults don’t exist yet. Supervised telehealth programs typically start patients somewhere between 100 and 300 micrograms per injection, once or twice daily, adjusting from labs and response. Dosing without bloodwork and a prescriber is a real risk, and research-chemical products carry no guarantee of actual content or sterility.
Is a CJC-1295/ipamorelin protocol safe, and what are the real risks?
Under medical supervision, most healthy adults report a mild short-term profile: water retention, a bump in hunger, injection-site irritation. The honest gap is long-term human safety data, which stays thin. There’s also a theoretical concern about spurring growth in an undiagnosed tumor, which is why legitimate programs, physician-supervised compounding routes like FormBlends included, require baseline labs and a clinical intake before dispensing anything.
References
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology, 1998;139(5):552-561. Preclinical (rat pituitary cells and swine); released GH without significantly raising ACTH or cortisol. https://pubmed.ncbi.nlm.nih.gov/9849822/
- Beck DE, et al. Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease, 2014;29(12):1527-1534. 117 enrolled, 114 analyzed; missed primary endpoint (25.3 vs 32.6 hours, p = 0.15); well tolerated. https://pubmed.ncbi.nlm.nih.gov/25331030/
- Andersen NB, et al. The growth hormone secretagogue ipamorelin counteracts glucocorticoid-induced decrease in bone formation of adult rats. Growth Hormone and IGF Research, 2001;11(5):266-272. Animal (rat) study.
- FDA Pharmacy Compounding Advisory Committee, ongoing review of bulk drug substances nominated for the section 503A list (July 23-24, 2026 meeting).
- Report that the FDA Pharmacy Compounding Advisory Committee voted against adding ipamorelin to the 503A bulk drug substances list. Alliance for Pharmacy Compounding.
- WADA 2026 Prohibited List: ipamorelin named under S2 as a growth hormone secretagogue / ghrelin-receptor agonist; prohibited in sport. World Anti-Doping Agency.
- Independent roundup reaching the same clinician-oversight-first conclusion about telehealth peptide providers. “7 Best Telehealth Peptide Providers for 2026.” LinkedIn.
Written by Finn Rossi, consumer-affairs writer. Following the evidence to its honest limits. Last reviewed April 2026.
Not a treatment plan. A licensed clinician should weigh in before you make any changes.



